Always Embarrassed by "Athlete's Foot" in Summer? Dermatologists Reveal 3 Methods to Treat Athlete's Foot
Summer is the peak season for athlete's foot, which can be an embarrassing time for some people. When visiting others' homes, they hesitate to take off their shoes, fearing that someone might mention an unpleasant odor, which can lead to sudden tension and blushing. In addition to its strong, fishy odor, athlete's foot often causes intense itching, making it an awkward issue in daily life.

1. What is athlete's foot?
n Athlete's foot, also known as Hong Kong foot, with the scientific name tinea pedis, is the most common infectious skin disease caused by dermatophytes and is highly contagious.
nCommon in adults and adolescents, particularly young males, and rarely occurs before puberty.
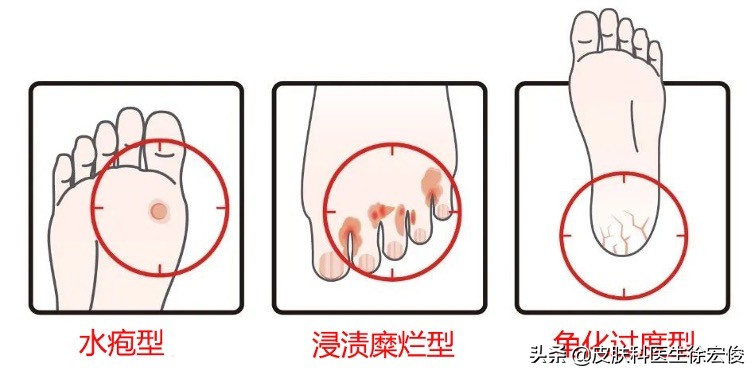
n Mainly manifests in three types:
1. Macerated and erosive type: The most common type, often occurring in the finger or toe webs. The skin becomes macerated and whitish, easily peeling off to leave a moist, erythematous, erosive surface with exudation, accompanied by an unpleasant odor.
2. Hyperkeratotic type: Involves the soles and inner and outer sides of the feet, characterized by dry skin, thickened keratin, deepened skin lines, and a tendency to crack.
3. Vesicular type: Commonly occurs on the palms and lateral aspects of the feet,Characterized by pruritic deep-seated vesicles that dry up after several days, presenting as a collarette of desquamation.
From the internet
2. The Hazards of Tinea Pedis
nInfecting oneself: Tinea pedis is often accompanied by onychomycosis, tinea cruris, or tinea manuum, which can result from adjacent infection or failure to separate laundry during washing.
nInfecting Others: Infection is typically caused by direct contact with pathogenic fungi, such as sharing shoes or socks, or walking barefoot in locker rooms or swimming pools.
nSecondary complications: Particularly in macerated and erosive tinea pedis, there is a high risk of secondary bacterial infections, as well as secondary acute lymphangitis, cellulitis, and erysipelas. When inflammation is significant, it can also easily lead to local eczematous changes or systemic dermatophytid reactions.
3. Treatment of Tinea Pedis
Topical treatment is the primary approach and the first choice for most patients, with a treatment course generally lasting 1 to 2 months. Topical medications include azoles, allylamines, butenafine, ciclopirox, and amorolfine. The selection of topical medications should be based on the classification of tinea pedis, with different treatment methods chosen accordingly.
1. For vesicular tinea pedis: choose a cream or solution with low irritation, such as ketoconazole, bifonazole cream or solution, etc.
2. For macerated erosive tinea pedis: Initially apply 3% boric acid solution or 0.1% rivanol solution for wet compress to reduce exudation. Once exudation decreases, apply powder such as miconazole powder. After the wound surface dries, apply a mild, low-irritation cream or ointment.
3. For hyperkeratotic tinea pedis: Preparations with strong exfoliating effects or high permeability can be selected, such as compound benzoic acid ointment or ciclopirox olamine. If necessary, occlusive therapy may also be employed to enhance efficacy.
nSystemic antifungal therapy is primarily used for patients who have failed local treatment, typically involving oral administration of terbinafine or itraconazole.
nIf secondary bacterial infection occurs, antibiotics should be combined; when dermatophytid is induced, antiallergic drugs may be administered.
4.Prevention of Athlete's Foot
For tinea pedis and tinea manuum, timely and thorough treatment is essential. If accompanied by onychomycosis, simultaneous treatment of onychomycosis is necessary to eliminate the source of infection. Additionally, it is important to develop good lifestyle habits, such as wearing breathable shoes and socks, and avoiding sharing personal items like footwear, socks, and foot basins.