Is cervical erosion really that scary? Doctor: 90% don’t need treatment; the two misconceptions to fear
Is cervical erosion really that scary?
。
“Doctor, I was diagnosed with severe cervical erosion! Am I about to get cancer? Should I rush to have laser surgery?” Every day in clinic I meet women terrified by the two words “erosion” — the term carries a frightening connotation of “serious lesion,” causing many to mistakenly think their cervix is “rotting,” and some private hospitals exploit this to sell “repair surgeries” costing thousands. Today, as a gynecologist, I want to make it clear: cervical erosion itself is not scary; 90% is a normal physiological phenomenon. What is truly dangerous is the panic that treats “erosion as cancer,” and the blind optimism that “ignores underlying pathology.”
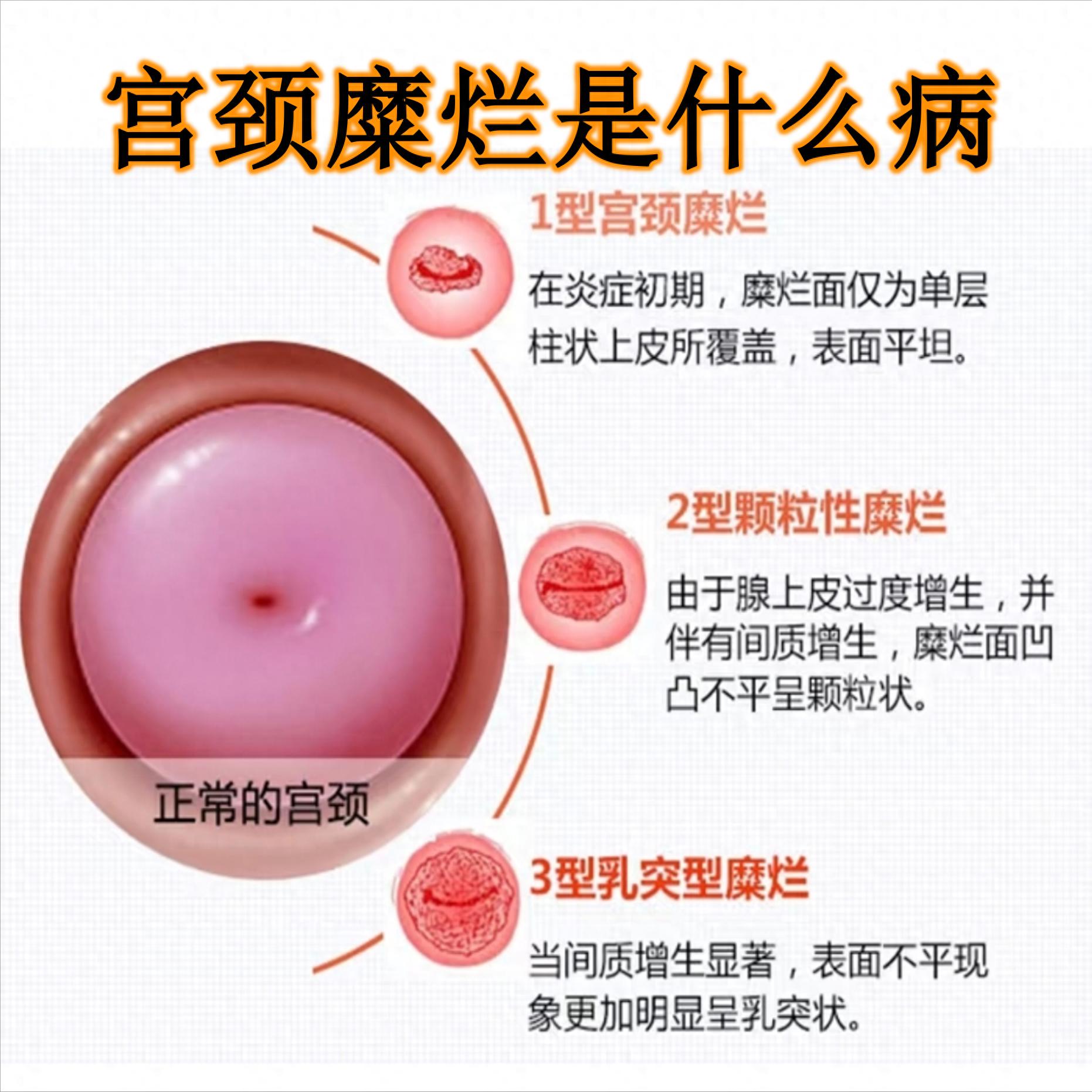
First, a reassurance: the term “cervical erosion” was removed from medical nomenclature in 2008. Its real identity is “cervical ectropion” — the cervix has two “skins,” the outer layer (squamous epithelium) is smooth, the inner layer (columnar epithelium) is red; when the inner layer extends onto the outer surface, it appears as “erosion” to the naked eye. In essence, this is a normal physiological change of the cervix and has nothing to do with cancer.
1. First, understand: why is it said that 90% of cervical erosion is not scary?
Physiological erosion: hormone-induced "normal displacement"
Young women, pregnant women, and those taking contraceptives have high estrogen levels, which "push" the columnar epithelium outward, producing "erosion-like changes." For example, 22-year-old college student Xiaomin had a physical exam that showed mild erosion, with normal TCT and HPV results. I told her no treatment was needed; two years later the "erosion" disappeared on re-examination — after hormone levels stabilized, the columnar epithelium gradually receded.
Asymptomatic erosion: no treatment or intervention needed
If "erosion" is found only on a physical exam and there are no symptoms such as increased vaginal discharge, postcoital bleeding, or lumbosacral/abdominal pain, and TCT and HPV tests are normal, no treatment is required whether the erosion is mild or severe. Clinical data show that women with this type of physiological erosion have the same cervical cancer risk as those without "erosion."
Treating the symptoms, not the erosion itself
Only when "erosion" is accompanied by cervicitis (for example, yellowish discharge, odor, postcoital bleeding) does it need treatment — what is treated is the inflammation, not the "erosion." For example, Ms. Zhang, age 30, had moderate erosion + bloody discharge; her routine vaginal smear showed bacterial cervicitis. After treating the infection with medication, the bleeding stopped and the "erosion" diminished. There was no need for physical treatments like laser or cryotherapy.
2. The two truly scary misconceptions that many fall into
Misconception 1: "Erosion = precursor to cancer, must have surgery"
This is the most harmful rumor! Aunt Li, age 45, was found to have severe erosion; a private hospital told her "if you don't operate now it will become cancer," so she paid 8,000 yuan for laser treatment, which resulted in cervical adhesions and severe menstrual pain. In fact, her TCT and HPV were completely normal — it was physiological erosion and did not require treatment. The surgery instead damaged the cervical mucosa and affected normal physiological function.
Misconception 2: "If erosion doesn't need treatment, then screening isn't necessary"
This is another fatal error! Behind a minority of "erosion-like changes" there may be hidden HPV infection or cervical lesions — for example, HPV16-positive low-grade cervical lesions can also appear as "erosion" to the naked eye. If not screened, they can slowly progress to high-grade lesions or even cervical cancer. Xiao Wang, 28, had mild erosion found during a physical exam and thought "no treatment needed" so he skipped screening. Three years later he experienced postcoital bleeding and was found to be HPV16-positive with high-grade lesions; fortunately, he underwent timely cone biopsy.
3. Practical guide: if cervical erosion is detected, what should you do?
Step one: Do these 2 tests to decide "whether to treat"
Whether mild or severe, first perform TCT (to examine cervical cells) and HPV (to detect oncogenic viruses):
If both tests are normal and the patient is asymptomatic → no treatment is needed; repeat annual check-up.
If both tests are normal but there is increased vaginal discharge or bleeding → treat the inflammation (use antibiotics or vaginal suppositories).
If TCT is abnormal or HPV is positive → proceed with colposcopy + biopsy to rule out lesions.
Step 2: Only in these situations should treatment be considered
Biopsy-confirmed cervical low-grade / high-grade lesion (this is treatment of the lesion, not of erosion);
Recurrent inflammation, severe leukorrhea with bleeding, affecting daily life (physical treatments such as microwave or laser may be used, but choose a reputable hospital).
Step 3: Avoid these 3 common scams
Don't believe "laser repairs erosion and prevents cancer" → Physiological erosion doesn't need repair; cancer is prevented through screening;
Don't buy "special gels for cervical erosion" → Gels can only relieve mild inflammation, they can't cure erosion, nor can they prevent cancer;
Don't be fooled by "severe is worse than mild" → The degree of erosion reflects only the extent of skin displacement, and is unrelated to pathology.
4. Final summary: Cervical erosion is not scary; doing one thing well is enough
Cervical erosion is like a "small misunderstanding of the cervix"; it is not a disease in itself and need not be feared. What should really be feared are "not undergoing screening" and "overtreatment." Remember:
If erosion is detected, first test TCT + HPV and let the test results speak;
If asymptomatic and exams are normal, live with peace of mind and have annual rechecks;
If symptomatic or exams are abnormal, provide targeted treatment—don’t be frightened by the two words "erosion."
As a gynecologist, I have seen too many women panic over "cervical erosion," and I have also seen cases where neglecting screening delayed treatment. The key to health is actually simple: do not panic blindly, and do not ignore screening. If you now have a report saying "cervical erosion," don't panic—first get TCT and HPV tests—most of the time you will receive the reassuring conclusion of "no treatment needed," and that is the most responsible choice for yourself!